Photoessay: The Skin and Diabetes Mellitus
by A Huntley
Dermatology Online Journal, December 1995
Volume 1, Number 2
Diabetes and Infection
candida
malignant external otitis
staph and strep
dermatophyte
candida infection
Candida albicans is a frequent pathogen in the skin of diabetics usually involving the groin or genital region. Candida involvement of the
groin region and uncircumcised penis tend to occur in men who have poor control of their diabetes.


Figs 35,36. Groin and genital region of 2 patients with diabetes mellitus demonstrating candida albicans infection. On the
left the groin region has erythema and multiple satellite papules, typical for candida infection of this region. On the right
the patient has erythema of the glans penis which is positive by potassium hydroxide examination for yeast.
The hands may also become involved with Candida. Usual sites of infection include proximal nail fold and intertriginous
areas which allow for natural moisture to accumulate. The finger web-space can serve as a moist area, and may be the site
of acute candida infection.

Fig 37. The web space between the third and fourth fingers on the left hand of this patient with diabetes mellitus demonstrates
erythema covered with a white curd-like material. A scraping of this material is positive for pseudohyphae on potassium hydroxide
examination.
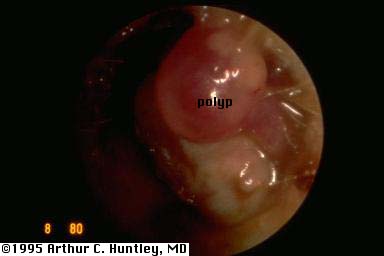
malignant external otitis
External otitis is a common enough diagnosis in the general population in general, however in diabetics it may become a serious
problem. The patient complains of severe ear pain from the otitis. The infection, due to Pseudomonas, may dissect along fascial planes and even gain access to cranial nerves. Examination of the ear canal reveals polypoid growths.
This infection has a mortality rate of about fifty percent.

Fig 38. Otoscopic view of Pseudomonas external otitis in an elderly diabetic patient. The polyp which is a characteristic
feature of malignant external otitis, is clearly visualized on the upper right wall.
staph and strep
Staphylococcus infection does not statistically account for more loss of work by diabetic employees. However, it seems that some of the
more severe infections encountered are in disabled patients.

Fig 39. Abscess involving the left arm of a diabetic patient. This patient developed a carbuncle at the site of insulin injection.

Fig 40. This patient has an ankle ulcer which developed an erythematous halo and a red streak going up the leg. This vascular
ulcer is complicated by cellulitis and lymphangitis.

Fig 41. First finger of a middle aged diabetic patient who complains of pain . The patient has acute bacterial paronychia
accompanied by lymphangitis.
dermatophyte infection
There are conflicting reports about an increased prevalence of dermatophyte infection in diabetics. For the population we
evaluated, the prevalence was not increased.

Fig 42. Dorsum of the left hand in a 25 year old diabetic student demonstrating an annular erythematous scaling plaque of
dermatophyte infection.
All contents copyright (C), 1995.
Dermatology Online Journal
University of California Davis