Lipedematous alopecia of the scalp
Published Web Location
https://doi.org/10.5070/D388n8z4m5Main Content
Lipedematous alopecia of the scalp
Bianca Maria Piraccini, Stylianos Voudouris, Massimiliano Pazzaglia, Giulia Rech, Colombina Vicenzi, and Antonella Tosti
Dermatology Online Journal 12 (2): 6
Department of Dermatology, University of Bologna, Via Massarenti 1, 40138-Bologna, Italy. tosti@med.unibo.itAbstract
Lipedematous scalp is a rare disorder, mainly described in adult African-American females. We report 2 adult caucasian males with lipedematous scalp associated with androgenetic alopecia. Patients were studied by dermoscopy and histopathology; they were treated with finasteride 1 mg. In our patients, lipedematous scalp affected the occipital and the vertex areas and pathologically exhibited mild edema and thickening of the adipose subcutaneous layer. At videodermoscopy, lipedematous scalp areas showed linear areas of teleangiectasia within the scalp creases, possibly caused by compression of the superficial blood capillaries by the increased volume of the subcutaneous fat layer within the thickened scalp. Finasteride at a dose of 1 mg per day for 1 year induced mild improvement of androgenetic alopecia in one patient and stabilization of the disease in the other. The lipedematous scalps remain unchanged. Lipedematous scalp is apparently a rare disease even though the condition is probably underdiagnosed. As a matter of fact, we diagnosed lipedematous scalp in our patients during a clinical examination for androgenetic alopecia, which was the patients' complaint. The association of lipedematous scalp and androgenetic alopecia in our two patients appears to be coincidental.
Introduction
Lipedematous scalp is a rare disease, mainly reported in black women, and is characterized by diffuse or circumscribed thickening of the scalp, more palpable than visible [1-12]. It can be associated with subjective symptoms, such as pain and pruritus, as well as with diffuse hair loss or inability of the hair on the thickened areas of the scalp to grow longer than a few centimeters. We describe two caucasian male patients who presented with lipedematous scalp associated with androgenetic alopecia. In one of the two patients, treatment with finasteride 1 mg produced hair regrowth.
Case reports
Case 1
 |
| Figure 1 |
|---|
| Vertex of our patient |
In July 2003 a 48-year-old healthy man presented to our clinic with a 10-year history of hair loss. Physical examination revealed Hamilton-IV androgenetic alopecia and a soft, cotton-like diffuse swelling of the scalp on the vertex (Fig. 1). The skin of the thickened scalp did not have signs of inflammation, and the patient was unaware of the abnormality. On palpation the scalp was thick, boggy, and had a spongy texture without fluctuation.
Case 2
In November 2003 a 53-year-old man, in good health, consulted us because of a 4-year history of diffuse hair loss associated with intermittent scalp itching. Physical examination revealed a Hamilton V vertex androgenetic alopecia and thickening of the scalp of the vertex and the occipital region. On palpation the scalp had a spongy texture without fluctuation. Videodermoscopy of the areas of scalp thickening revealed in both cases linear areas of erythema along the scalp creases. The erythematous areas showed fine arborizing telangiectasia and small coiled capillary loops (Figs. 2a, 2b). Both patients submitted to a scalp biopsy. Vertical and horizontal sections were performed.
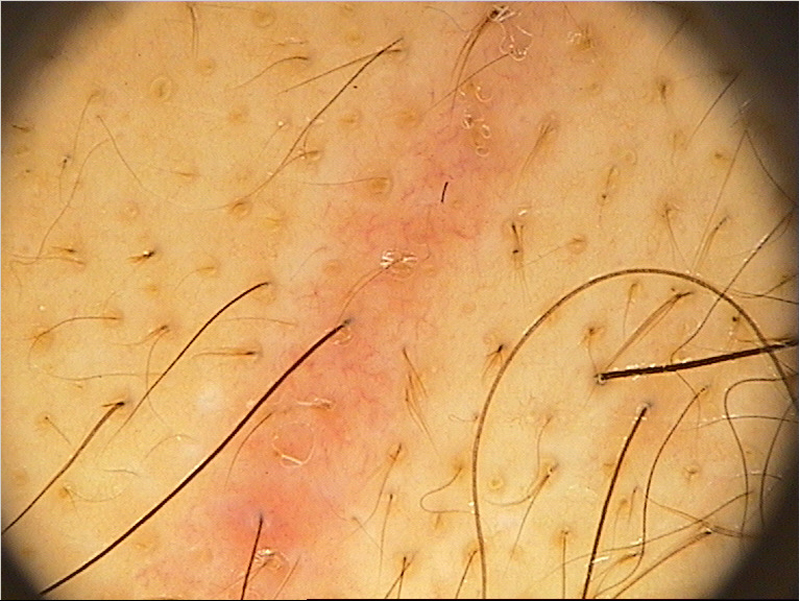 |  |
| Figure 2a | Figure 2b |
|---|---|
| Figures 2a and 2b. Videodermoscopy at 20x (2a) and 40x (2b) revealed an erythematous area with fine arborizing telangiectasia and small coiled capillary loops. | |
 |
| Figure 3 |
|---|
| Normal hair density with a reduced terminal-to-vellus ratio. No inflammatory changes. The subcutaneous adipose tissue is thickened and mildly edematous. |
The microscopic examination showed normal hair density with a reduced terminal-to-vellus ratio (3:1 in the first patient and 2.5:1 in the second). No inflammatory changes were detected. The subcutaneous adipose tissue was thickened and mildly edematous (Fig. 3). No accumulation of mucin within the dermis or subcutaneous matrix could be detected. As measured from the biopsy slide, scalp thickness from the uppermost layer of the stratum corneum to the soft tissue was 11mm in the first patient and 12 mm in the second (normal value = 5-6 mm).
The clinical features and the histopathologic findings of our patients led us to the diagnosis of lipedematous scalp associated with male pattern androgenetic alopecia.
Both patients were treated with finasteride 1mg/day. The 1-year followup assessed by global photography and digital videodermoscopy of the scalp showed no changes of the lipedematous scalp in both patients and a mild improvement of androgenetic alopecia in the first patient. The androgenetic alopecia of the second patient remained stable.
Discussion
In 1935 Cornbleet was the first to describe a thickening of the subcutaneous fat layer of the scalp [1, 2]. Since then, fewer than 20 similar cases have been reported in the literature [1-11]. Diffuse or localized thickening of the scalp without hair loss is called lipedematous scalp, and has been reported in four cases, all adult females [3, 9, 10, 11, 12].
The term lipedematous alopecia was first introduced in 1961 by Coskey et al. [2], who described shortening of the hair over the thickened scalp in two patients. Lipedematous scalp may be associated both with inability of the hair of the thickened scalp to grow longer than a few centimeters and with diffuse hair loss [1, 2, 4, 5, 6, 7, 10]. When hair loss is present, the term lipedematous alopecia is preferred to better describe the clinical features. Both lipedematous scalp and lipedematous alopecia have been reported predominantly in African-American healthy women.
Scalp thickening is usually localized at the vertex and occipital areas and may slowly expand to the entire scalp. Pain and itching of the thickened areas may be associated. The diagnosis depends upon the clinical features and on pathology, which shows thickening of the subcutaneous adipose tissue of the scalp. Both MRI and head ultrasound scan can be useful to identify and measure the increased scalp thickness.
The pathogenesis of lipedematous scalp and the associated alopecia are not known. Some authors report the presence of edema of the thickened adipose tissue [6, 8, 10] and dilated lymphatic vessels [10] and suggest that lymphangiectasia may be responsible for hair loss because it is found only in those patients with lipedematous scalp and alopecia. The two cases we reported are adult caucasian males with lipedematous scalp, very uncommon for their race and sex. They both exhibited androgenetic alopecia. They are the first patients with lipedematous scalp studied by dermoscopy, which showed striking and exclusive features, consisting in vascular abnormalities restricted to the areas of scalp thickening. In fact in both patients at videodermoscopy, the lipedematous scalp areas presented linear areas of telangiectasia within the scalp creases. This was possibly caused by compression of the superficial blood capillaries by the increased volume of the subcutaneous fat layer within the thickened scalp. This finding is not related to androgenetic alopecia, because it has never been described in this disease [13]. Neither lymphatic nor blood vessel dilation was seen in the biopsies of our patients and we could not make a correlation between dermoscopic and pathological features.
The association of lipedematous scalp and androgenetic alopecia in our two patients is, in our opinion, coincidental and resulting from the high frequency of androgenetic alopecia in men. The fact that the lipedematous scalp coincided with the areas affected by androgenetic alopecia is possibly related to the fact that both conditions tend to be localized in the vertex. The casual correlation of lipedematous scalp and androgenetic alopecia in our patients is furthermore suggested by results of treatment with finasteride 1 mg. One year of finasteride treatment in fact induced improvement of androgenetic alopecia in one patient and stabilization in the other, but it did not affect the lipedematous scalp, which remained unchanged in both cases.
Lipedematous scalp is apparently a rare disease even though the condition is probably underdiagnosed. Most of the reported cases so far have been females. We diagnosed lipedematous scalp in our male patients during a clinical examination for androgenetic alopecia, their presenting concern.
References
1. Coskey RJ, Fosnaugh RP, Fine G. Lipedematous alopecia. Arch Dermatol. 1961 Oct;84:619-22. PubMed2. Curtis JW, Heising RA. Lipedematous alopecia associated with skin hyperelasticity. 1964 Jun;89:819-20. PubMed
3. Lee JH, Sung YH, Yoon JS, Park JK. Lipedematous scalp. Arch Dermatol 1994Jun;130(6):802-3. PubMed
4. Kane KS, Kwan T, Baden HP, Bigby M. Women with new-onset boggy scalp. Arch Dermatol. 1994 Jun;130(6):802-3. PubMed
5. Bridges AG, von Kuster LC, Estes SA. Lipedematous alopecia. Cutis. 2000 Apr;65(4):199-202. PubMed
6. Fair KP, Knoell KA, Patterson JW, Rudd RJ, Greer KE. Lipedematous alopecia: a clinicopathologic, histologic and ultrastructural study. J Cutan Pathol. 2000 Jan;27(1):49-53. PubMed
7. Ikejima A, Yamashita M, Ikeda S, Ogawa H. A case of lipedematous alopecia occurring in a male patient. Dermatology. 2000;201(2):168-70. PubMed.
8. Tiscornia JE, Molezzi A, Hernandez MI, Kien MC, Chouela EN. Lipedematous alopecia in a white woman. Arch Dermatol. 2002 Nov;138(11):1517-8. PubMed.
9. Scheufler O, Kania NM, Heinrichs CM, Exner K. Hyperplasia of the subcutaneous adipose tissue is the primary histopathologic abnormality in lipedematous scalp. Am J Dermatopathol. 2003 Jun;25(3):248-52. PubMed
10. Martìn JM, Monteagudo C, Montesinos E, Guijarro J, Llombart B, Jordà E. Lipedematous scalp and lipedematous alopecia: a clinical and histologic analysis of 3 cases. J Am Acad Dermatol. 2005 Jan;52(1):152-6. PubMed
11. High WA, Hoang MP. Lipedematous alopecia: an unusual sequela of discoid lupus, or other co-conspirators at work? J Am Acad Dermatol. 2005 Aug;53(2 Suppl 1):S157-61. PubMed
12. Cornbleet T. Cutis verticis gyrata? Lipoma? Arch Dermatol Syph 1953; 32: 688.
13. Lacarrubba F, Dall'Oglio F, Rita Nasca M, Micali G. Videodermatoscopy enhances diagnostic capability in some forms of hair loss. Am J Clin Dermatol. 2004;5(3):205-8. PubMed
© 2006 Dermatology Online Journal