The Clinical Diagnosis of Early Malignant Melanoma: Expansion of the ABCD Criteria to Improve Diagnostic Sensitivity
Published Web Location
https://doi.org/10.5070/D366x188mbMain Content
The Clinical Diagnosis of Early Malignant Melanoma: Expansion of the ABCD Criteria to Improve Diagnostic Sensitivity
Brent P. Hazen1, Ashish C. Bhatia2, Tarif Zaim3,
and Robert T. Brodell4
Dermatology Online Journal 5(2): 3
1.Albion College, Albion, Michigan2.Northeastern Ohio Universities College of Medicine
3.Veterans Administration Medical Center, Cleveland
4.Northeastern Ohio Universities College of Medicine and Case Western Reserve University School of Medicine
Abstract
With the steady increase in incidence of malignant melanomas (MM) in the United States, early diagnosis and complete removal are critical for the containment of the malignancy.[1] The "ABCD" method of identification, originally described by Friedman et al., has been a useful tool in facilitating the diagnosis of MM.[2,3,4] This method analyzes four clinical characteristics to identify a malignant melanoma: Asymmetry, Border irregularity, Color variegation, and a Diameter of 6 mm or more.[4] Clinicians recognize that some melanomas lack all or most of the features defined in the "ABCD" rules.[5] This may be especially true of some early invasive and in situ melanomas.[6,7] In these instances, clinical history documenting morphologic change over time can be an important additional consideration. The following case reports underscore the need to expand the ABCD mnemonic to include an "E" for "Evolutionary change." An additional modification is also needed to emphasize the need for a low threshold for biopsy of unusual lesions which do not show typical benign features, even if they do not meet the ABCDE criteria. To this end we propose an "F" for "Funny looking lesions".
Case Reports


Discussion
Physician detection of melanoma during physical examination has been shown to result in detection of thinner melanomas when compared to patient detection, spouse detection, or detection by other means.[8] These thinner melanomas are associated with improved outcomes.[9] The educated eye of the physician is important, but the fact remains that the diagnosis of malignant melanoma is difficult for many physicians.[5] In a study by Grin et al, diagnostic sensitivity for melanomas was 84.5 0.000000rom 1974 to 1982 and lower in years prior.[10]
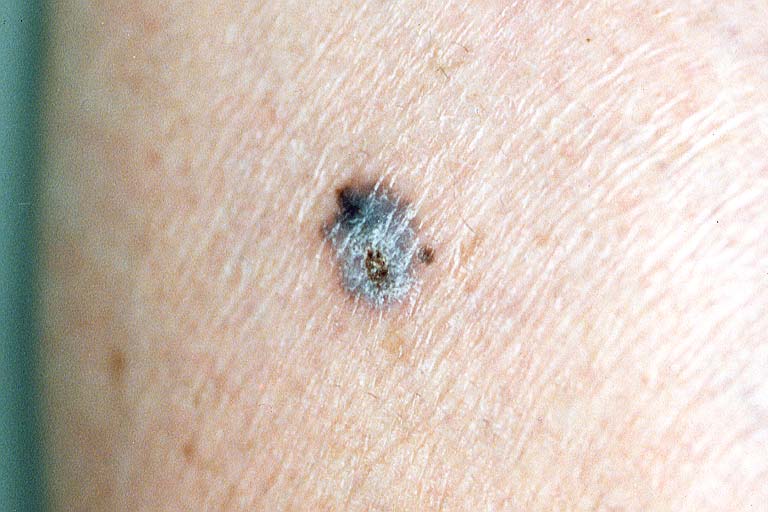
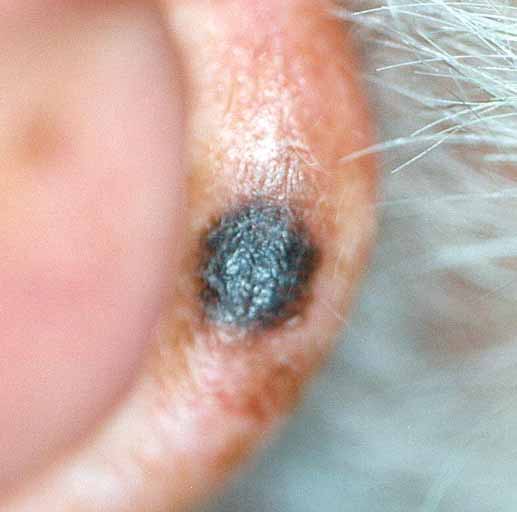
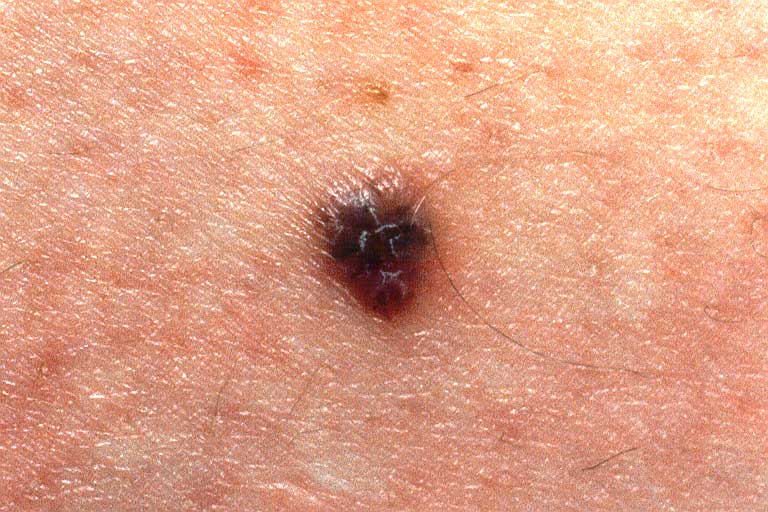
The "ABCD" method has proven to be useful in the diagnosis of malignant melanoma. It has been particularly beneficial because the mnemonic is easily remembered by physicians and lay persons alike. However, as seen in our patients, dependence on these criteria alone may fail to identify all melanomas. The history of physical changes, namely in color and size in Case 1 and Case 2, recent crusting in Case 3, and increase in size in Case 4 and 5, were the principal features which led to biopsy and histopathologic study demonstrating malignant melanoma. (Table I).
A history of recent evolution or "changing" in a nevus has been documented as a key to the diagnosis of melanoma. The American Cancer Society included a "change in a mole" as one of its "Seven Warning Signs of Cancer" in a major public education campaign. The importance of evolutionary changes in detecting melanoma is particularly important in small, early, and in situ melanomas where traditional "ABCD" criteria are often inadequate to make a clinical diagnosis.[11] Many types of physical and historical changes have been described. Anderson and Silvers have suggested that rapid growth and altered pigmentation may be important clinical features in diagnosing melanomas.[5] Wick et al have also noted that changes in size and color are key features in early diagnosis, being found in 71% (size) and 55% (color) respectively of Clark's Level II tumors.[11] Other features such as bleeding, tenderness, itching, and loss of skin markings may also be found in lesions of melanoma, but these "changes" are less helpful since they are most often seen in late or extensive tumors.[11,12]
For these reasons we favor adding an "E" to the ABCD mnemonic for the diagnosis of malignant melanoma. An original "E" proposal called for adding "Elevation",[13] however, many benign nevi are elevated. We believe Rigel's "E" - "Enlarging at a faster rate than neighboring lesions" emphasizes important historical features of early malignant melanoma.[14] However, our "E", "Evolutionary Changes", encompasses changes in color (including surrounding erythema and hyperpigmented halo), size, symmetry, surface characteristics, pruritis, pain, bleeding, and tenderness. This is more inclusive of the various historical changes cited in the cases above.
After further analysis, we realized that there were physical features of several of these lesions, which were hard to quantify, except in a negative fashion. They did not appear to be typically benign nevi, cherry hemangiomas, seborrheic keratoses, or other benign cutaneous changes. Additionally the suspect lesions often appeared different from other benign lesions seen in the same patient, i.e. the Ugly Duckling sign.[15] Intuitive diagnosis by experienced clinicians has been shown to be highly sensitive when compared to standardized criteria in the diagnosis of another dermatologic neoplasm, common viral warts.[16] We believe these intuitive qualities can also be critical in the early diagnosis of malignant melanoma. For this reason, we have added an "F" to the ABCDE mnemonic to describe "Funny-looking lesions". Such lesions should be biopsied and submitted for pathologic examination even when other criteria might be absent. Cases 2 and 3 show subtle features, which might trigger a biopsy based on their "funny-looking" appearance.
Additional surface topographical features may be identified by using technological assists such as serial photography, ultrasonography, epiluminescence microscopy, computer-based expert systems, and dermatoscopy.[17,18,19] However, inspection using standardized guidelines still must be used to identify which lesions might be subjected to additional testing. Additionally, the lack of availability and the need for special training with these technologies, limit their usefulness. Kittler et al recommend adding an "E" which includes morphologic change to the ABCD rule for epiluminescence microscopy (dermatoscopy).[20]
Of course, the experience of the observer is also a critical factor in the diagnosis of malignant melanoma. In Cassileth et al, only 140f non- dermatologists successfully identified five of six melanomas, while 690f dermatologists correctly identified the tumors.[1] We recognize however that some melanomas will defy diagnosis by even the most astute clinician applying all physical diagnostic and historical criteria.[21]
In summary, our report supports the need for applying historical features - "Evolutionary changes", and less specific physical diagnostic factors - "F" (Funny-looking lesions) to increase the sensitivity of the "ABCD" criteria for the diagnosis of malignant melanoma (Table 1). We recognize that increasing the sensitivity of the ABCD criteria will decrease the specificity, but feel this is warranted in a disease where a late diagnosis can lead to death. It is our hope that the "ABCDEF's" of melanoma will serve as a useful diagnostic and teaching tool which will have an impact on early diagnosis of melanoma and save lives.
Table I. Summary of case presentations using the ABCDEF method for diagnosis| Feature | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 |
| A -Asymmetry | +/- | +/- | - | - | - |
| B -Border | +/- | - | - | - | - |
| C -Color | - | - | +/- | - | - |
| D -Diameter | - | - | +/- | - | - |
| E -Evolutionary changes | + | + | + | + | + |
| F-Funny | - | + | + | - | - |
+: Feature present in patient
-: Feature absent in patient
References
1. Cassileth BR, Clark WH, Lusk EJ, et al. How well do physicians recognize melanoma and other problem lesions? J Am Acad Dermatol 4:555-60, 1986.
2. Dial WF. ABCD rule aids in preoperative diagnosis of malignant melanoma. Cosmetic Dermatol 8(3):32-4, 1995.
3. Friedman RJ, Rigel DS, Kopf AW. Early detection of malignant melanoma: the role of physician examination and self-examination of the skin. CA Cancer J Clin May-Jun;35(3):130-51, 1985 .
4. Friedman RJ, Rigel DS, Silverman M, Kopf AW. The continued importance of early detection of malignant melanoma. CA, 41:201-26, 1991.
5. Anderson WK, Silvers DN. Melanoma? It can't be melanoma! JAMA 266(24):3463-5, 1991.
6. Schneider JS, Moore II DH, Sagebiel RW. Early diagnosis of cutaneous malignant melanoma at Lawrence Livermore National Laboratory. Arch Derm 126:767-9, 1990.
7. Koch SE, Henneberry JM. Clinically subtle primary cutaneous melanoma. J Am Acad Dermatol 40:252-4. 1999.
8. Epstein DS, Lange JR, Gruber SB, Mofid M, Koch SE. Is physician detection associated with thinner melanoma? JAMA 281:640-3, 1999.
9. Breslow A. Thickness, cross-sectional areas, and depth of invasion in the prognosis of cutaneous melanoma. Ann Surg. 172:902-8, 1970.
10. Grin C, Kopf A, Welkovich B, Bart R, Levenstein M. Accuracy in the clinical diagnosis of melanoma. Arch Dermatol 126:763-6, 1990.
11. Wick MM, Sober AJ, Fitzpatrick TB, Mihm MC, et al. Clinical characteristics of early cutaneous melanoma. Cancer 45:2684-6, 1980.
12. Lederman JS, Fitzpatrick TB, Sober AJ. Skin markings in the diagnosis and prognosis of cutaneous melanoma. Arch Dermatol 120:1449-52, 1984.
13. Fitzpatrick TB, Rhodes AR, Sober AJ, et al. Primary malignant melanoma of the skin: the call for action to identify persons at risk; to discover precursor lesions; to detect early melanomas. Pigment Cell 9:110-7, 1988.
14. Rigel DS, Friedman RJ. The rationale of the ABCDs of early melanoma. J Am Acad Dermatol 29(6):1060-1, 1993.
15. Grobb JJ. The 'Ugly Duckling' sign: Identification of the common characteristics of nevi in an individual as a basis for melanoma screening. Arch Derm 134:103-4, 1998.
16. Young R, Jolley D, Marks R. Comparison of the use of standardized diagnostic criteria and intuitive clinical diagnosis in the diagnosis of common viral warts (verrucae vulgaris). Arch Dermatol 134:1586-9, 1998.
17. Rivers JK. Melanoma. Lancet 347:803-6, 1996.
18. Argenziano G, Fabbrocini G, Carli P, DeGiorgi V, Sammarco E, Delfino M. Epiluminescence microscopy for the diagnosis of doubtful melanocytic skin lesions. Arch Dermatol 134:1563-70, 1998.
19. Steiner A, Pehamberger H, Wolff K. In vivo epiluminescence microscopy of pigmented skin lesions and early detection of malignant melanoma. J Acad Dermatol 17(4):582-3, 1987.
20. Kittler H, Seltenheim M, Dawid M, Pehamberger H, Wolff K, Binder M. J Morphologic changes of pigmented skin lesions: a useful extension of the ABCD rule for dermatoscopy. J Am Acad Dermatol 40:558-562, 1999.
21. Grant-Kels J, Bason E, Grin C. The misdiagnosis of malignant melanoma. J Am Acad Dermatol 40:539-48, 1999.
© 1999 Dermatology Online Journal